Tearing in childs
What are the causes tearing in the child?
In any child with tearing we need to ask several questions: age of onset, tearing characteristics and accompanying symptoms.
Tearing in the newborn: We must first rule out neonatal infections as a cause. Tearing attributable to these causes is rare due to current prophylaxis.
Always explore the presence of congenital malformations such as epiblepharon eyelid, distichiasis and entropion, all of which can lead to tearing.
Once the aforementioned conditions are ruled out, the main cause of tearing in the newborn is the blockage of the tear ducts.
The lacrimal drainage system begins in the puncta located on each eyelid, the two are joined by a canaliculus which flows into the lacrimal sac, from here it flows into the bone through the nasolacrimal duct before emptying into the nostril. Thus the tear travels from the eye to the nose and throat continuously.
In newborns there is often some kind of membrane in the mouth of the lachrymal in the nose, where there is a small valve (of Hassner) that prevents the normal flow of tears, causing tearing (epiphora).
Lacrimal obstruction is common in infants, and can affect up to 50% of newborns. In the first months of life the lacrimal duct unfolds, and from the second month of life the percentage of obstruction is less than 5%.
During the first year of life the majority of children will heal and only a small percentage will eventually require treatment.
Every child with tearing should be seen and treated by an ophthalmologist from the onset of symptoms. The success of probing is related to age, and in children over 3 years the chances of effective treatment are significantly lower.
Sometimes there are family conditions that could explain differential anatomical facts, which are repeated in the same family. Often the mother relates that she too had a weeping eye.
What are the symptoms?
The main symptom is watery secretion that can be constant or just occasional: the latter case appears when exponed to the wind, in the street, with the sun... Tearing may cause irritation of the skin of the eyelids.
 |
| Tearing in the left eye, eyelid inflammation |
Conjunctivitis can also be accompanied with abundant secretion or even dacryocystitis (inflammation of the lacrimal sac).
 |
|
| Acute dacryocystitis |
|
 |
 |
| Dacryocystitis. Evolution with antibiotic treatment | |
How is blockage of the tear ducts in the child treated?
The aim is to unlock that somehow possible obstruction permeabilising the pathway.
Parents should understand that there are imaging tests to find out exactly what the problem is. We suspect that the valve is imperforate and its expansion will improve symptoms. But it does not always have to be this way. Sometimes anomalous duct stricture the mouth or in the nose is not correct, or is blocked by any small alteration nose, which can cause probing failure.
Therefore treatments are aimed at delaying the passage and for this we follow a protocol based on the child's age.
Until 9 months to one year of age, massage is the recommended treatment. Parents should be advised to gently massage the lacrymal area longitudinally moving the finger towards the wing of the nose, to increase hydrostatic pressure in the lower area and break the valve. These massages should be performed about 10 times, morning and evening.
 |
| Massage direction |
After the first year probing of the lacrymal duct is considered.. This probing often can be performed without anesthesia. However it is advisable to do it with general anesthesia. Parents should take a low anesthetic risk but the technique is more comfortable for the child and also the surgeon has time to check your result.
Occasionally probing can be done in patients less than 8-9 months, in those who are symptomatic.
Probing of the lacrymal duct is a very common and delicate procedure that must be performed by experienced professionals. Used metal probes are inserted through the punctum and go all the way along its route and directions to reach the nose. This in theory causes breakage and dilation of the valve. Being a maneuver practised in a blind manner, there is a low risk of harming the lachrymal duct, so it is not completely risk free.
 |
 |
 |
 |
 |
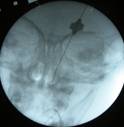 |
| Lacrimal probing sequence. Fluoroscopy showing the position of the probe | ||
This technique is very quick and can take less than one minute.
Afterwards we verify successful opening of the pathway by irrigation and checking its output in the nostril or endoscopically.
Recovery is immediate. The child may attend the nursery the next day.
Generally antibiotic eye drops are prescribed to be applied for three days.
Following this procedure the child may have some tears and bloody nasal mucus.
Another review is conducted monthly.
The success rate is 90%.
Probing is always performed as a first attempt, including children aged 4-5 years, although in these cases the success rate decreases.
In cases of failure a second catheterization can be performed one month after the first.
If probing fails: In these cases another procedure is performed: Intubation of the lacrimal duct. With this procedure, a tube is placed inside the silicone lacrymal duct, which is left for a period of 6-12 months.
It is performed under general anesthesia. Punctal silicone probes are introduced to reach the nose where they are knotted and housed. The process can sometimes last several minutes depending on the anatomy of the nostril and the type of pipes used.
These tubes do not usually give any problems, they are barely visible. Parents and the child should be instructed not to traction them in the only point where they are displayed.
 |
| Intubation partially emerged due to pulling |
For removal sedation if often used.
Success is achieved in 90% of cases.
An alternative to intubation is dacryocystoplasty with Lacricath ©. This is a new procedure in which a tube is inserted in the lacrimal metal. This tube is threaded into a deflated balloon. Once located in the area the ball swells with a manometer, thus expanding and breaking the closed valve. A probe is then removed.
 |
It is a more expensive procedure than intubation with similar effectiveness. The advantage is that the tubes are left inside the lacrimal duct.
If intubation fails: The last alternative is the dacryocystorhinostomy. We usually wait until 3-5 years to perform it. The technique is the same as that used in adults. (See Tearing in adults). The purpose is to create a new pathway surgically between the lacrimal sac and the nose.
There are two ways: by endoscopic or external approach. Each has its advantages and disadvantages.
This surgery is performed under general anesthesia and usually a requires hospitalization for one day. The child will have a plugged nose for 24-48 hours.
The results of this surgery you get few children are very good, definitely solving your problem in 90% of cases.